Surgery for uterine cancer can remove the visible tumour, but not always the invisible threat. Clean reports can still hide microscopic disease.
A uterine cancer doctor recommends radiation therapy when surgery cannot eliminate residual or high-risk cells, helping reduce recurrence and improve survival. In aggressive stages or post-surgical risk, radiation is not optional; it is control. Those unseen pelvic cells can return stronger if ignored.
Today’s blog will discuss when radiation is necessary when surgery alone is not enough.
So, let’s dive in.
Why surgery sometimes ‘isn’t enough’
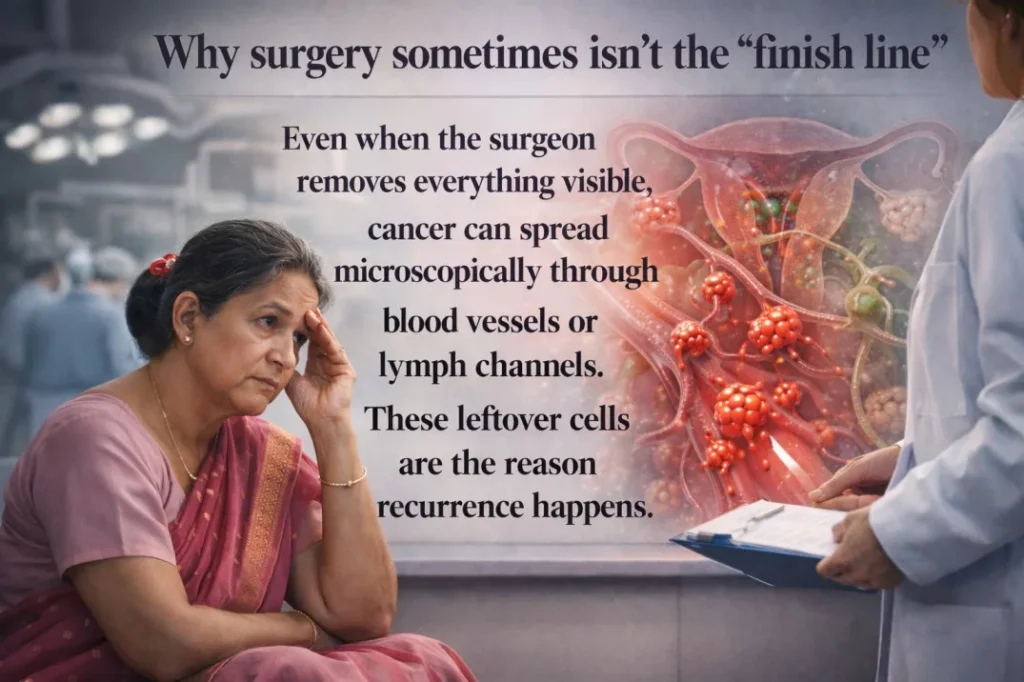
Surgery removes the visible tumour, but microscopic cancer cells may remain in nearby tissues or lymph nodes. If high-risk indicators are found in the pathology report, additional treatment like radiation may be needed to reduce recurrence risk. After a hysterectomy, the removed tissue is examined carefully.
The pathologist studies
- How deeply the tumour invaded the uterine muscle
- Whether lymph nodes were involved
- And whether the cancer was close to the surgical margins
Radiation is not a sign that surgery failed. It is a protective step taken when risk is higher than average.
Quick basics—what radiation therapy actually does in uterine cancer
Radiation therapy uses high-energy beams to destroy remaining cancer cells after surgery. It reduces the risk of pelvic cancer recurrence and improves long-term disease control in selected patients.
The goal (kill leftover cells, reduce recurrence risk)
The goal of radiation therapy for uterine cancer is simple and scientific:
- Destroy microscopic cancer cells
- Reduce pelvic recurrence
- Improve survival in high-risk cases
In many patients, especially those with aggressive features, endometrial cancer radiation significantly lowers local relapse rates.
When it’s used (after surgery vs before surgery vs for recurrence)
Radiation may be used:
- After surgery as part of uterine cancer treatment after surgery
- Rarely before surgery in selected cases
- For recurrence when cancer returns
When doctors recommend radiation after a hysterectomy
Radiation after hysterectomy is recommended when pathology shows high-risk features, lymph node involvement, or incomplete tumour removal. It is used to reduce recurrence and improve disease control.
Many women ask, when is radiation needed after a hysterectomy? The answer lies in the pathology report.
High-risk features on biopsy/pathology report
- Deep myometrial invasion
- Higher-grade tumour
- Cervix involvement
- Lymphovascular space invasion (LVSI)
- Positive or close margins
Refer to the table
| High-Risk Feature | Why It Matters |
| Deep invasion | Higher chance of spread |
| High grade | Faster-growing cancer |
| LVSI | Spread through vessels |
| Positive margins | Residual disease risk |
These cases often require high-risk endometrial cancer adjuvant therapy, which includes radiation.
Lymph node involvement and advanced stages
If lymph nodes are positive, the disease is no longer limited. In uterine cancer, stage 2 and stage 3 radiation, pelvic radiation becomes crucial to control the disease locally.
When surgery isn’t possible or doesn’t remove everything
In medically unfit patients or when residual tumour remains, radiation may act as primary treatment. At this stage, expert guidance from a uterine cancer doctor in Kolkata becomes extremely important to avoid under-treatment or over-treatment.
Types of radiation used for uterine cancer (and how to choose)
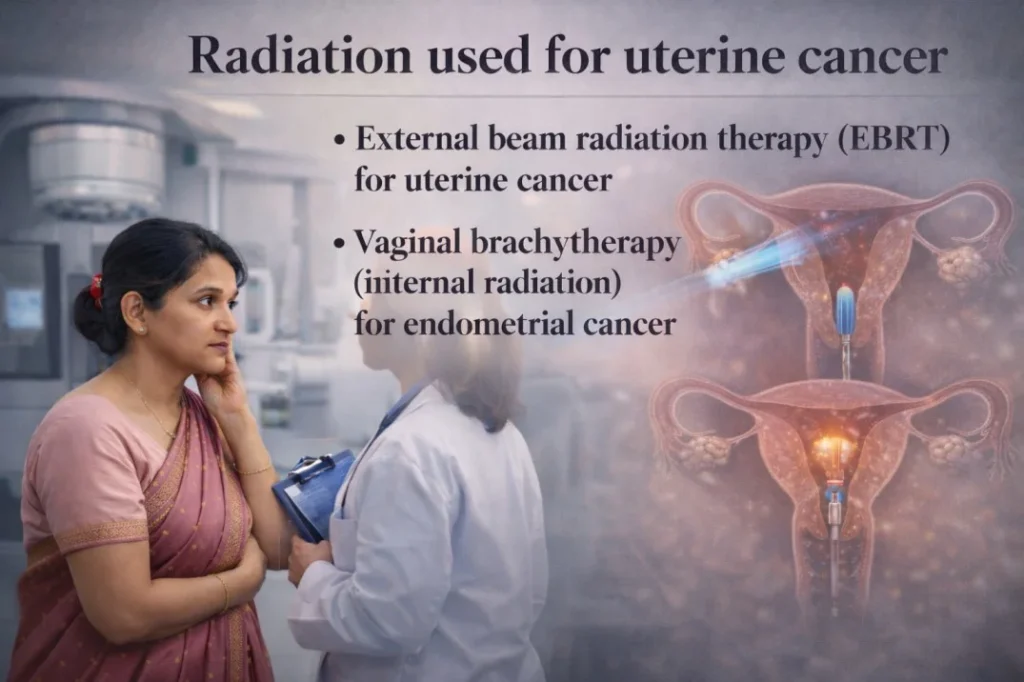
Two main types are used: external beam radiation and vaginal brachytherapy. The choice depends on stage, pathology findings, and overall health.
External Beam Radiation Therapy (EBRT)
External beam radiation therapy (EBRT) for uterine cancer delivers radiation from outside the body to the pelvis.
It targets:
- Pelvic lymph nodes
- Vaginal vault
- Areas at risk
Treatment usually lasts 4–5 weeks.
Vaginal brachytherapy (internal radiation)
Vaginal brachytherapy for endometrial cancer places a radiation source inside the vagina for a few minutes per session. It is focused and limits exposure to the bladder and bowel.
EBRT + brachytherapy (when both are advised)
EBRT + brachytherapy is advised together when uterine cancer shows high-risk or residual disease. EBRT treats the pelvis broadly, while brachytherapy delivers targeted radiation to the tumour site, ensuring deeper control and lowering recurrence risk.
| Clinical Situation | Radiation Strategy |
| Early-stage, high-risk | Brachytherapy (focused internal radiation) |
| Lymph node involvement | EBRT ± brachytherapy |
| Advanced local spread | EBRT + brachytherapy (combined approach) |
Treatment is individualised. This decision should be taken carefully. The good news is that Dr Mukti Mukherjee, an experienced uterine cancer doctor in Kolkata, understands risk stratification properly and guides patients down the right treatment plan.
Radiation vs chemo vs both—what’s the difference?
Radiation treats cancer locally in the pelvis. Chemotherapy circulates throughout the body. Some patients need one; others need both based on stage and risk factors.
When radiation is preferred
- Cancer is confined to the pelvis
- The risk of local recurrence is high
- The patient cannot tolerate chemotherapy
When chemo is added
- Lymph nodes are positive
- The tumour is aggressive
- Risk of distant spread exists
This comparison of radiation vs chemotherapy for uterine cancer is not about choosing one over the other. It is about choosing what your disease biology demands.
Common combinations
- Chemotherapy followed by radiation
- Concurrent chemo-radiation
- Sequential therapy
The ultimate aim is uterine cancer recurrence prevention.
What the treatment plan looks like (step-by-step)
Radiation treatment involves planning scans, precise mapping, and daily sessions over several weeks. It is painless and carefully monitored.
Planning scan + mapping (simulation)
A CT simulation scan is done. We map the exact target area. Organs like the bladder and rectum are protected.
Precision is everything.
Treatment schedule
| Type | Duration |
| EBRT | 5 days/week for 4–5 weeks |
| Brachytherapy | 2–5 sessions |
| Combined | As advised |
What you feel during sessions
You feel nothing during radiation delivery. No burning. No shock. Simply put, it is painless, and nothing dramatic happens.
Side effects—what’s common, what needs a quick call
Most side effects are temporary and manageable. Serious complications are uncommon with modern radiation techniques.
Short-term side effects
Most women experience these common pelvic radiation side effects:
- Fatigue
- Bowel/bladder changes
- Mild loose stools
- Frequent urination
- Skin irritation
These improve after treatment.
Vaginal dryness/tightness and intimacy concerns
Vaginal dryness and tightness after radiation can affect comfort and intimacy. Understanding brachytherapy side effects and recovery allows the timely use of
- Moisturisers
- Dilator therapy
- And gentle pelvic exercises
These help restore flexibility, reduce discomfort, and support long-term sexual health and quality of life after uterine cancer treatment.
Red-flag symptoms
Seek medical advice if you notice:
- Heavy bleeding
- Severe pain
- High fever
- Persistent vomiting
Early reporting prevents complications.
Recovery and follow-up after radiation
Recovery is gradual. Most women resume normal activity within weeks. Regular follow-up is essential to detect recurrence early.
Diet + hydration basics during pelvic radiation
During pelvic radiation, the bowel and bladder become sensitive, so simple eating habits make a big difference. Drink adequate water throughout the day. Good hydration protects the bladder, reduces burning during urination, and supports faster recovery.
Choose light, home-cooked meals such as rice, dal, curd, soft vegetables, and easily digestible foods. Avoid very spicy, fried, or oily foods, as they can worsen loose motions or acidity.
Work, travel, and daily routine
Most women can continue light household work or desk jobs during treatment since radiation sessions are short and you are not radioactive afterwards.
Fatigue is common, so pace yourself. Take short rest breaks and avoid overexertion. Travel is usually safe when necessary, but long, tiring journeys are best postponed until treatment is completed.
Follow-up schedule and recurrence monitoring
Typically:
- Every 3–4 months for the first 2 years
- Every 6 months after that
- Annual visits later
Regular review with a uterine cancer doctor in Kolkata ensures proper long-term monitoring.
Chances of control/recurrence—what patients should realistically know
Radiation significantly reduces pelvic recurrence in high-risk patients, but outcomes depend on stage, grade, and lymph node status.
Early-stage patients receiving appropriate adjuvant treatment often achieve excellent control rates. Advanced stages need combined therapy and close monitoring. There are no guarantees in oncology. But evidence-based treatment dramatically improves outcomes.
Timely consultation with Dr Mukti Mukherjee, an experienced uterine cancer doctor in Kolkata, makes a real difference in survival and quality of life.
People Also Ask
Is radiation necessary for stage 1 uterine cancer?
Not always. Low-risk stage 1 cases may not need it. High-risk features may require radiation.
What is vaginal brachytherapy, and does it hurt?
It is internal radiation delivered inside the vagina. It is usually painless and quick.
How long does radiation take after a hysterectomy?
External radiation takes about 4–5 weeks. Brachytherapy may require a few additional sessions.
Can I have radiation if I’m older or have diabetes/BP?
Yes. Age and controlled medical conditions are not automatic barriers. Each case is assessed individually.
Will radiation affect urination or bowel movements permanently?
Most changes are temporary. Permanent problems are uncommon with modern techniques.
Can uterine cancer come back after surgery? How does radiation help?
Yes, recurrence is possible. Radiation kills remaining microscopic cells, significantly reducing that risk.
The Main Takeaway
Radiation is not an extra treatment. It is a protective treatment. Women who benefit most include:
- High-grade tumours
- Deep invasion
- Node-positive disease
- Close surgical margins
If you have undergone surgery, bring your full pathology report. Do not rely on assumptions.
Consult Dr Mukti Mukherjee, a dedicated uterine cancer doctor in Kolkata, for personalised guidance. Her expertise in modern radiation planning ensures accurate treatment with safety.
Book a session today without hesitation.